

The Challenges of Phyllodes Tumours of the Breast.
About the Patient and condition
A 27-year-old lady (newly married), had a long-standing lump in her right breast which was evaluated elsewhere. An ultrasound scan of the breast indicated it to be an encapsulated, hypoechoic lesion 32mmx23mm in size. A Fine Needle Aspiration Cytology (FNAC) indicated it to be a Fibro Epithelial Lesion, very likely to be a Fibroadenoma. The patient opted for conservative treatment with regular follow up.
After 3 months, there was an increase in size and an ultrasound scan showed the lesion to be 8mmx53mmx51mm in size, partially solid and partially cystic, with moving echoes and surrounding oedema. The Radiologist’s impression was that the Fibroadenoma now had cystic degeneration and surrounding inflammation.
Case Scenario
At this point of time, the patient presented to Dr. Uma Krishnaswamy, Consultant Breast & Oncoplastic Surgeon at Apollo Hospitals, Chennai. Examination revealed a 10cmsx10cms tender, cystic mass in the right breast adjacent to the Nipple Areola Complex, extending from the 6 O’clock to the 9 O’clock sectors with extensive skin bruising. The clinical diagnosis was highly suggestive of a Giant Fibroadenoma with degeneration and a post FNAC induced unresolved haematoma. The second diagnosis was a Phyllodes tumour of the breast, possibly malignant.
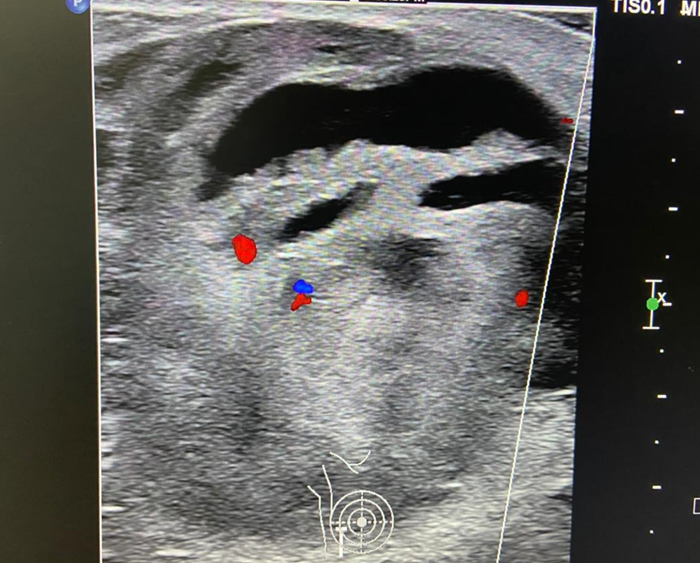
Routine preoperative blood parameters revealed no coagulation abnormality. An ultrasound scan examination was undertaken as part of the Triple Diagnostic pathway. This revealed a 66mmx53mm, partially well defined, encapsulated, solid cum cystic mass with Brownian movement. Colour Doppler showed minimal internal vascular flow. Once again, the Radiology findings were suggestive of a degenerating Fibroadenoma with surrounding haematoma.
This was followed up in the same sitting with an Image guided Core Needle biopsy. 60ml of frank, fresh blood was aspirated with immediate refilling, preventing the Interventional Radiologist from proceeding to the biopsy for fear of hemorrhage. This event gave rise to the possibility that it was an Intracystic papillary lesion with bleeding or a Phyllodes tumour.
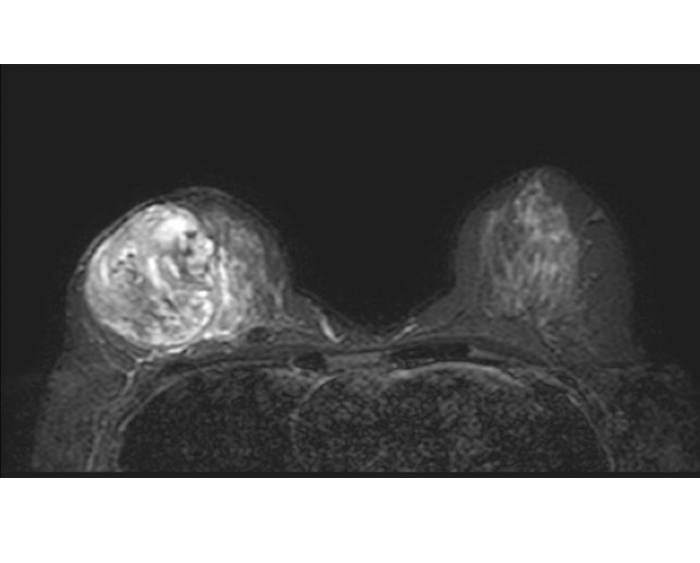
Pursuing the diagnostic pathway, an MR Mammogram was undertaken. This showed an encapsulated and hetero intense lesion with possible necrotic and hemorrhagic content. There was no additional diagnostic information to be had.
Worldwide Scenario
The surgical management of Phyllodes tumours of the Breast, whether benign or malignant, is fraught with challenges. The disease is a well-established one, with an incidence less than 1% of all breast tumours. There are, however, major challenges in the preoperative diagnosis and differentiation between a Benign Phyllodes and a Malignant Phyllodes, though benign lesions are more common. This challenge is compounded by the surgical technique to be utilized to excise them with a clear margin to prevent recurrence, as well as preserve the cosmesis of the breast. This is particularly important as Phyllodes tumours occur in a relatively young age group (25-30 years) in Asian populations with a preponderance in women and rarely in men with Gynaecomastia.
Expertise at Apollo Hospitals
After general and anaesthetic evaluation, the patient was taken up for surgery with informed consent. The findings were that of a partially encapsulated, necrotic mass with old blood and clots, with surrounding inflammatory fat and oedema. A wide excision of the mass was done. To fill the volume deficit, an Intra mammary Flap Reconstruction was done. The patient was discharged after 24 hours.
Histopathology examination showed a 9x6x4 cms solid cum cystic mass with dark red friable material. Microscopy showed a neoplastic lesion with epithelium lined spaces and a spindle cell stroma with scattered mitosis and clear margins. (Figure 3).
Immuno histochemistry examination revealed: Ki67 value of 7 and p53 to be negative. The impression hence was a Phyllodes of borderline grade with low malignant potential. As a Genomic panel for Fibroepithelial lesions is currently not available commercially in India it was not pursued.
Apollo Hospitals – Touching Lives
The Multidisciplinary team at Apollo Hospitals decided to proceed with Radiotherapy. On completion of the same, the patient remains under close surveillance. Patient satisfaction was high as there has been no recurrence of the Phyllodes tumour to date and the cosmetic result has been excellent.
Patient’s testimonial
Patient was satisfied with the services and treatment offered at Apollo Hospitals.
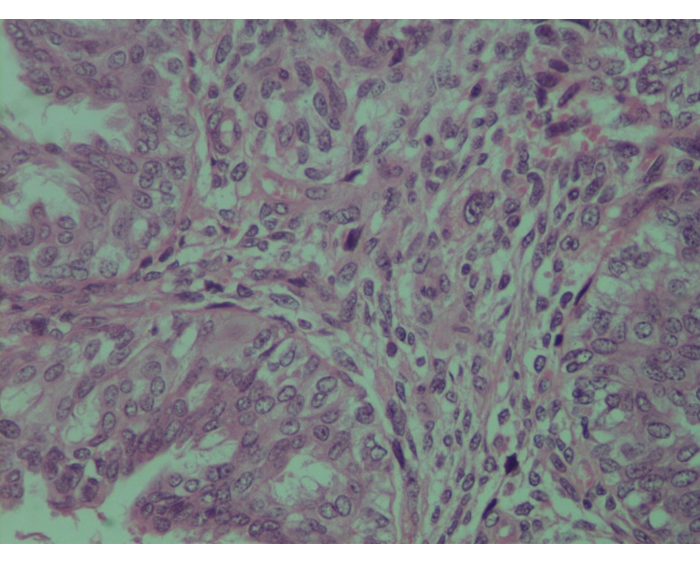
epithelium and increased stromal cellularity and atypia
(x400 magnification)


