-
Emergency
-
Apollo Lifeline
-

Emergency
Emergency
![]() Verified By June 11, 2023
Verified By June 11, 2023
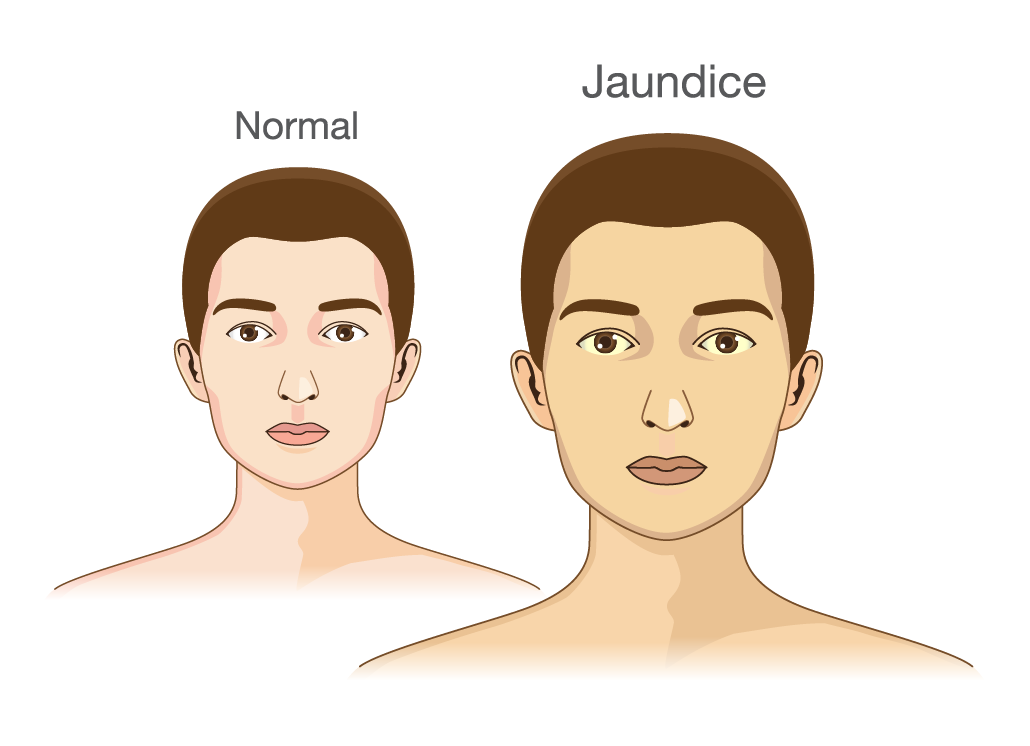
Jaundice, also known as icterus, is a yellowish pigmentation of skin and sclera of the eyes and mucous membranes due to high bilirubin levels in the body.
The word Jaundice is derived from a French word called “jaunisse”, meaning “yellow disease”. The yellowish discoloration is due to bilirubin (a fluid secreted by the liver). Breakdown of RBC’s, leads to the formation of bilirubin in our body. Bilirubin is normally metabolized in the liver and excreted in the bile from our body. The disruption in the metabolism, production or excretion of bilirubin leads to deposits of an excess amount of bile in the body, causing jaundice. Due to their high elastin content, the white of the eye has a particular affinity towards bilirubin. Serum bilirubin would be at least 3 mg/dL in scleral icterus.
Jaundice is of 3 types such as
A) HEPATOCELLULAR JAUNDICE (HEPATIC): It is usually caused by infections, drugs and alcohol.
B) HEMOLYTIC JAUNDICE (PRE-HEPATIC): occurs due to the destruction of RBC’s and overproduction of bilirubin.
C) OBSTRUCTIVE JAUNDICE (POSTHEPATIC): It is caused by infections, alcohol, cirrhosis, lymphoma, pregnancy, cirrhosis, tumors.
In Newborns, jaundice is very commonly seen in the first week of life after birth and reduces within 2 weeks of life. If the bilirubin levels are greater than 4-20mg/dL, it can be treated with phototherapy. Exchange transfusions are done in severe cases. Kernicterus can occur if bilirubin levels in babies are very high for a prolonged period and may lead to brain damage.
Ultrasound, CT scan, and MRI imaging are useful medical imaging to identify the cause of jaundice. Both medical and surgical management is done depending on the severity of the condition causing jaundice. Medical management involves the treatment of underlying infections. Surgical treatment is preferred in cases of obstructive jaundice.
Jaundiceis caused due to to high bilirubin levels in the body known as hyperbilirubinemia. In blood, the normal levels of bilirubin are less than 1.0 mg/dL and levels above 2–3 mg/dL result in Jaundice.
1) UNCONJUGATED BILIRUBIN (INDIRECT): It is usually seen in newborn jaundice, thyroid disorders, fasting for a long time, and in Genetic conditions like Gilbert’s Syndrome.
2) CONJUGATED BILIRUBIN (DIRECT): It is commonly seen in viral hepatitis c and cirrhosis (liver diseases), blockage of the bile duct (caused due to gallstones blocking the hepatic ducts and in pancreatitis), infections of the liver and medications.
1) Pre-hepatic Cause (before the bile is produced by the liver): The conditions that cause increased breakdown of red blood cells than the normal process like sickle cell crisis, malaria, thalassemia, drugs and other toxins.
2) Hepatocellular Cause: The transportation of the bilirubin across the hepatocytes (cells in liver) is interrupted at any point between the cellular uptake of unconjugated bilirubin and transportation of conjugated bilirubin into bile ducts. It is caused by hepatitis, alcoholic liver disease, liver cancer and paracetamol overdose.
3) Post-Hepatic Cause (after the liver produces the bile): The normal drainage of bile (conjugated bilirubin) from the liver into the intestines is interrupted in obstructive jaundice. The conditions that cause obstructive jaundice are gallstones in the bile ducts, cancers of gall bladder/ bileduct, cholangitis (infections of the bileduct), pancreatitis(infections of the pancreas), pregnancy and newborn jaundice. This is commonly associated with dark colored urine, pale stools (clay colored stools) and Itchiness of the body. Severe Itching is seen often in patients with elevated serum cholesterol levels.
Physiological Jaundice, Breast milk jaundice, breast feeding jaundice, cephalohematoma and Maternal -fetal blood group incompatibility are also a few causes of jaundice.
4) Incompatibility of Maternal-fetal blood group (ABO, Rh): The rapid breakdown of red blood cells of the fetal blood due to incompatibility between the blood groups of the mother and the fetus causes jaundice due to high bilirubin levels in the body.
1) DUBLIN-JOHNSON SYNDROME: This is an inherited disorder of chronic jaundice resulting in conjugated hyperbilirubinemia secondary to a defect in the canalicular transport of organic anions. Serum bilirubin levels may rise upto 30 mg/dL. Usually, no treatment is required.
2) CRIGLER-NAJJAR SYNDROME: It is also an inherited disorder caused by a mild deficiency in UDPGT enzyme. Serum unconjugated bilirubin levels are in the range of 6-25mg/ dl. Treatment includes usage of phenobarbitone, UV light and liver transplantation.
3) PSEUDO-JAUNDICE: It is usually caused by excessive consumption of beta-carotene containing foods like carrot, pumpkin, or melons. It is usually harmless and leads to yellowish discolouration of the skin.
Common symptoms include yellowish colored skin and sclera, usually starting from the head and spreads down the body (sclera has more affinity towards bilirubin), dark or brown colored urine, pale stools(clay colored stools due to absence of bile pigments in stools), itchiness (pruritis and excoriation are seen in severe cases caused by the bile salts present in the bile). Other symptoms include abdominal pain, fatigue and myalgia, weight loss, fever and vomiting.
The symptoms of jaundice vary depending on the cause and the underlying diseases from one individual to individual.
Jaundice occurs due to hyperbilirubinemia (High levels of Bilirubin in the blood). Often underlying diseases or disorders are the main cause. These prevent the liver from getting rid of bilirubin from the body and it gets deposited in the tissues.
Some of the common underlying disorders that require treatment are bile duct obstruction ( Bilirubin levels increase in the body due to Obstruction in liver), Gilbert’s Syndrome ( Bile excretion from the body is impaired as enzymes that are involved in this process are affected. It is an inherited disorder), Hemolytic Anemia (when RBC’s are broken down in large amounts, then the Bilirubin production in the body is increased), Bile duct Inflammation and acute inflammation of the liver. In cholestasis, the bile flow from the liver is interrupted hence conjugated bilirubin remains in the body.
If viral hepatitis is suspected, risk factors include intravenous drug abuse, blood transfusions, the exposure to blood or body fluids of an infected person and multiple sexual partners.
Risk factors also include ingestion of potential toxins i.e certain drugs like paracetamol (overdose causes liver failure), solvents(chemicals) and wild mushrooms.
Jaundice is usually diagnosed by symptoms, history given by the patient and physical examination.
1) A physical examination is usually done to look for signs and symptoms of jaundice. Swelling of the liver, ankles and feet that suggests Cirrhosis or Scarring of the liver. Liver is felt hard on examination by a doctor (on palpation).
2) The medical history of the patient must include whether the patient has travelled recently to any country or region where hepatitis or malaria is prevalent, if the patient is an alcoholic or there is any recent use of alcohol by the patient, any recent history of drug abuse like paracetamol and occupational hazards(whether he is exposed to any harmful chemicals that can affect the liver in his workplace).
BILIRUBIN TEST: protein levels such as total protein and albumin and LIVER FUNCTION TESTS can be done to confirm Jaundice.
BILIRUBIN TEST: The levels of bilirubin in a blood test is called a bilirubin test. It measures the indirect or unconjugated bilirubin levels in the body.
In blood, the Normal Levels of bilirubin are less than 1.0 mg/dL (17 µmol/L) and levels above 2–3 mg/dL (34-51 µmol/L) result in Jaundice.
In Haemolytic Jaundice, high levels of unconjugated bilirubin is seen. Increased Heme metabolism can be seen and increased levels of urine-urobilinogen (> 2 units) can be seen with no bilirubin. Unconjugated bilirubin is not water-soluble, hence cannot be observed in the urine but it is seen only in serum. The only exceptions are newborns and infants as the gut flora has not yet developed.
LIVER FUNCTION TESTS: ALP (alkaline phosphatase), GGT and ALT, AST (aminotransferases) tests can be done.
Normal levels are ALP (10–45 IU/L), GGT (18–85IU/L), AST (12–38 IU/L) and ALT (10–45 IU/L).
In obstructive jaundice, all four of them are very high. In cases of acute hepatocellular damage, AST levels are 15 times more than the normal value and lesser values indicate obstructive causes. ALP levels that are 10 times the normal value are seen in CMV (CYTOMEGALOVIRUS ) or chronic hepatitis infections. In Acute Hepatitis, ALT and AST levels are above (1000 IU/L). ALT and AST levels are around (1500-2250 IU/L) in Acetaminophen toxicity. GGT levels that are 5 times the normal value indicate drug toxicity.
Jaundice can be prevented by
Yes, Jaundice can be cured. If it is caused due to underlying infection, your doctor may suggest medical management. But in severe cases and if it occurs due to obstruction, then surgery is suggested.
Jaundice is serious only when bilirubin levels are very high in the body and it may cause complications like liver failure, sepsis and death.
The treatment of jaundice depends on the underlying conditions. In newborns, it disappears after 2 weeks of life.
Apollo Hospitals has the Best Gastroenterologist in India. To find the best gastroenterologist doctors in your nearby city, visit the links below: