-
Emergency
-
Apollo Lifeline
-


Emergency
Jaundice
![]() Verified By Apollo Hospitals June 12, 2019
Verified By Apollo Hospitals June 12, 2019
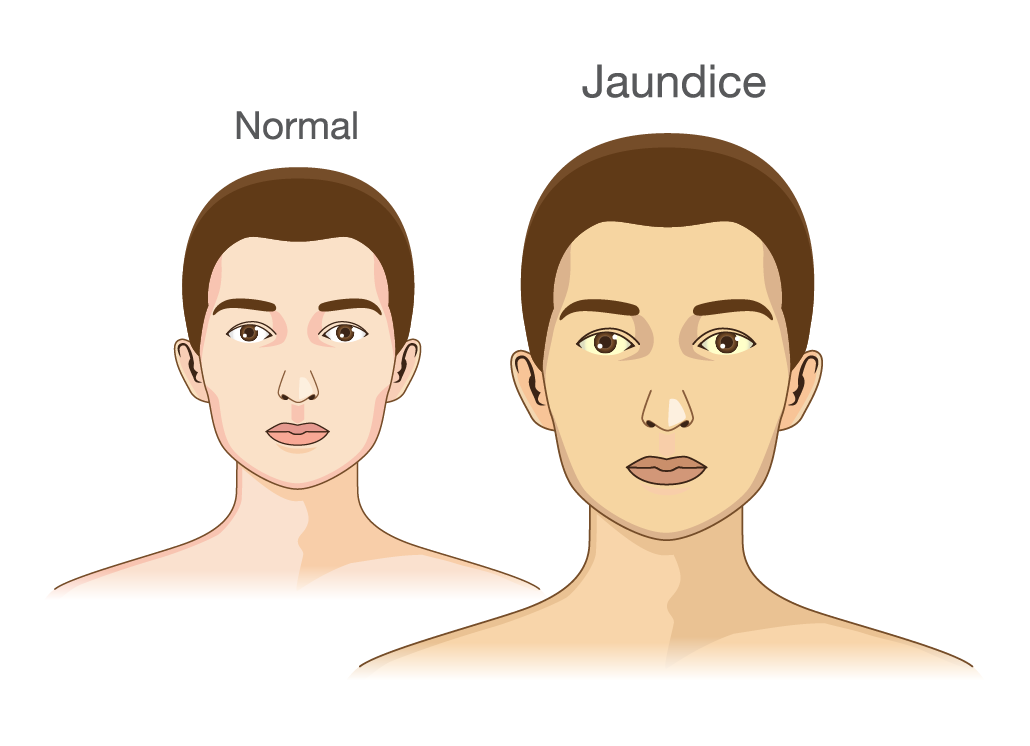
Jaundice, also known as icterus, is the yellowish pigmentation of skin and sclera of the eyes and mucous membranes due to high bilirubin levels in the body.
The word Jaundice is derived from a French word called “jaunisse”, meaning “yellow disease”. The yellowish discolouration is due to Bilirubin (a fluid secreted by the liver). Breakdown of RBC’s, leads to the formation of Bilirubin in our body. Bilirubin is normally metabolized in the liver and excreted in the bile from our body. The disruption in the metabolism, production or excretion of Bilirubin leads to deposits of an excess amount of bile in the body, causing Jaundice. Due to their high elastin content, the white of the eye has a particular affinity towards Bilirubin. Serum bilirubin would be at least 3 mg/dL in scleral icterus.
Jaundice is caused due to high bilirubin levels in the body known as hyperbilirubinemia. In blood, the normal levels of Bilirubin are less than 1.0 mg/dL and levels above 2–3 mg/dL result in Jaundice.
Bilirubin can be of 2 types:
1) UNCONJUGATED BILIRUBIN (INDIRECT): It is usually seen in newborn Jaundice, thyroid disorders, fasting for a long time, and in Genetic conditions like Gilbert’s Syndrome.
2) CONJUGATED BILIRUBIN (DIRECT): It is commonly seen in viral hepatitis and cirrhosis (liver diseases), blockage of the bile duct (caused due to gallstones blocking the hepatic ducts and in pancreatitis), infections of the liver and medications.
Often Jaundice is caused by various underlying disorders that require treatment, such as:
1) Pre-hepatic Cause (before the bile is produced by the liver): The conditions that cause an increased breakdown of red blood cells than the normal process like sickle cell crisis, malaria, thalassemia, drugs and other toxins.
2) Hepatocellular Cause: The transportation of the Bilirubin across the hepatocytes (cells in the liver) is interrupted at any point between the cellular uptake of unconjugated Bilirubin and transportation of conjugated Bilirubin into bile ducts. It is caused by Hepatitis, alcoholic liver disease, liver cancer and paracetamol overdose.
3) Post-Hepatic Cause (after the liver produces the bile): The normal drainage of bile (conjugated Bilirubin) from the liver into the intestines is interrupted in obstructive Jaundice. The conditions that cause obstructive Jaundice are gallstones in the bile ducts, cancers of gall bladder/ bileduct, cholangitis (infections of the bileduct), pancreatitis(infections of the pancreas), pregnancy and newborn Jaundice. This is commonly associated with dark colored urine, pale stools (clay colored stools) and Itchiness of the body. Severe Itching is seen often in patients with elevated serum cholesterol levels.
Physiological Jaundice, Breast milk jaundice, breast feeding jaundice, cephalohematoma and Maternal -fetal blood group incompatibility are also a few causes of Jaundice.
- Physiological Jaundice: It is most commonly seen in newborns and appears in the first week of life. The rapid breakdown of red blood cells that occur at this age cannot be processed by the immature liver of the newborn. Bilirubin remains in the body causing Jaundice but it is harmless and gradually reduces within the first 2 weeks of life.
- Breast milk jaundice: A harmless form of Jaundice that occurs at the end of first week of life after birth. It is believed to be caused by certain chemicals present in the breast milk. Breast feeding must be stopped for 1-3 days. Phototherapy can be given. It may rarely lead to Kernicterus.
- Breastfeeding jaundice: Seen in the newborns who are not properly breast fed by the mother’s milk. The inadequate intake of breast milk in newborn leads to fewer bowel movements causing decreased bilirubin excretion from the body.
- Cephalohematoma: It is caused due to injury to the head of the baby during delivery. The blood gets collected under the scalp and rapid breakdown of these red blood cells can cause a surge in the bilirubin levels in the body, causing Jaundice.
4) Incompatibility of Maternal-fetal blood group (ABO, Rh): The rapid breakdown of red blood cells of the fetal blood due to incompatibility between the mother and fetus blood groups causes Jaundice to high bilirubin levels in the body.
Other conditions that may cause jaundice includes
1) DUBLIN-JOHNSON SYNDROME: This inherited chronic Jaundice disorder results in conjugated hyperbilirubinemia secondary to a defect in the canalicular transport of organic anions. Serum bilirubin levels may rise up to 30 mg/dL. Usually, no treatment is required.
2) CRIGLER-NAJJAR SYNDROME: It is also an inherited disorder caused by a mild deficiency in UDPGT enzyme. Serum unconjugated bilirubin levels are in the range of 6-25mg/ dl. Treatment includes usage of phenobarbitone, UV light and liver transplantation.
3) PSEUDO-JAUNDICE: It is usually caused by excessive consumption of beta-carotene containing foods like carrot, pumpkin, or melons. It is usually harmless and leads to yellowish discolouration of the skin.
Common symptoms include yellowish colored skin and sclera, usually starting from the head and spreads down the body (sclera has more affinity towards Bilirubin), dark or brown colored urine, pale stools(clay colored stools due to absence of bile pigments in stools), itchiness (pruritis and excoriation are seen in severe cases caused by the bile salts present in the bile). Other symptoms include abdominal pain, fatigue and myalgia, weight loss, fever and vomiting.
The symptoms of Jaundice vary depending on the cause and the underlying diseases from one individual to individual.
- Pre-Hepatic Causes: Patients experience abdominal pain, weight loss and fatigue due to increased breakdown of red blood cells in diseases like malaria, sickle cell crisis and thalassemia. In hemolytic Jaundice, an enlarged spleen is seen.
- Hepatocellular Cause: Symptoms like Dark colored urine, pale stools and itching are seen in cases of viral Hepatitis. In alcoholic liver disease, the patient may have severe abdominal pain and discomfort, gastritis and fatigue. In liver cancers and paracetamol overdose, symptoms may vary depending on the prognosis of the patient. In cirrhosis or scarring of the liver, the patient will have portal hypertension.
- Post-Hepatic Cause (after the liver produces the bile): Symptoms like yellowish discolouration of skin, pale stools, abdominal pain, weight loss, malaise are seen in Obstructive Jaundice caused by gallstones diseasein the bile ducts, cancers of gallbladder/ bileduct, cholangitis (infection of the bileduct), pancreatitis(infection of the pancreas), pregnancy and newborn Jaundice. In cases of choledocholithiasis, fever and tenderness in the abdomen are present. Painless Jaundice is seen in malignant biliary obstruction.
Jaundice occurs due to hyperbilirubinemia (High levels of Bilirubin in the blood). Often underlying diseases or disorders are the main cause. These prevent the liver from getting rid of Bilirubin from the body and it gets deposited in the tissues.
Some of the common underlying disorders that require treatment are bile duct obstruction ( Bilirubin levels increase in the body due to Obstruction in liver), Gilbert’s Syndrome ( Bile excretion from the body is impaired as enzymes that are involved in this process are affected. It is an inherited disorder), Hemolytic Anemia (when RBC’s are broken down in large amounts, then the Bilirubin production in the body is increased), Bile duct Inflammation and acute inflammation of the liver. In cholestasis, the bile flow from the liver is interrupted hence conjugated Bilirubin remains in the body.
If viral Hepatitis is suspected, risk factors include intravenous drug abuse, blood transfusions, the exposure to blood or body fluids of an infected person and multiple sexual partners.
Risk factors also include ingestion of potential toxins i.e certain drugs like paracetamol (overdose causes liver failure), solvents(chemicals) and wild mushrooms.
Jaundice is usually diagnosed by symptoms, history given by the patient and physical examination.
1) A physical examination is usually done to look for signs and symptoms of Jaundice. Swelling of the liver, ankles and feet that suggests Cirrhosis or Scarring of the liver. Liver is felt hard on examination by a doctor (on palpation).
- In the liver cancers, liver is rock-hard on touch.
- In haemolytic Jaundice, Splenomegaly (enlarged spleen) is felt on palpation.
- In cases of malignant biliary obstruction, the patient does not have any abdominal pain or tenderness and is commomly known as painless Jaundice.
- Excoriation is seen in cholestasis and high grade biliary obstruction.
- Greenish Hue (due to biliverdin) can be seen in a few cases that suggests long standing liver conditions like biliary cirrhosis, sclerosing cholangitis, severe chronic Hepatitis or long standing malignant obstruction.
- If fever and tenderness in the abdomen are present it suggests Cholestasis, choledocholithiasis.
- Palmar Erythema (Redness in palms) may suggest chronic ethanol ingestion.
- In viral Hepatitis, flu like symptoms can be seen even before the Jaundice occurs in the patient.
2) The medical history of the patient must include whether the patient has travelled recently to any country or region where Hepatitis or malaria is prevalent if the patient is an alcoholic or there is any recent use of alcohol by the patient, any recent history of drug abuse like paracetamol and occupational hazards (whether he is exposed to any harmful chemicals that can affect the liver in his workplace).
Tests
BILIRUBIN TEST: The levels of Bilirubin in a blood test is called a bilirubin test. It measures the indirect or unconjugated bilirubin levels in the body.
In blood, the Normal Levels of Bilirubin are less than 1.0 mg/dL (17 µmol/L) and levels above 2–3 mg/dL (34-51 µmol/L) result in Jaundice.
In Haemolytic Jaundice, high levels of unconjugated Bilirubin are seen. Increased Heme metabolism can be seen and increased levels of urine-urobilinogen (> 2 units) can be seen with no bilirubin. Unconjugated Bilirubin is not water-soluble, hence cannot be observed in the urine but it is seen only in serum. The only exceptions are newborns and infants as the gut flora has not yet developed.
LIVER FUNCTION TESTS: ALP (alkaline phosphatase), GGT and ALT, AST (aminotransferases) tests can be done.
Normal levels are ALP (10–45 IU/L), GGT (18–85IU/L), AST (12–38 IU/L) and ALT (10–45 IU/L).
In obstructive Jaundice, all four of them are very high. In cases of acute hepatocellular damage, AST levels are 15 times more than the normal value and lesser values indicate obstructive causes. ALP levels that are 10 times the normal value are seen in CMV (CYTOMEGALOVIRUS ) or chronic hepatitis infections. In Acute Hepatitis, ALT and AST levels are above (1000 IU/L). ALT and AST levels are around (1500-2250 IU/L) in Acetaminophen toxicity. GGT levels that are 5 times the normal value indicate drug toxicity.
- c) CBC (Complete Blood Count): It shows the level of Red Blood Cells, White Blood Cells, and Platelets in blood.
- d) Tests to Identify the liver infections can also be done such as Hepatitis A, B, C & E tests.
- e) Urine tests can be done to measure the levels of urobilinogen. Lower levels of urobilinogen suggest post-hepatic causes and higher levels suggest pre or intrahepatic causes.
- f) In suspected cases for Obstruction, Imaging can be done like MRI, CT scans, and Ultrasound. ULTRASOUND can be used to identify the Blockage of the Bile ducts and Gall bladder.
- g) Liver Biopsy (a needle is inserted into the liver and tissue sample is taken out which is examined under the microscope) is suggested in cases of fatty liver, cancer, cirrhosis, and inflammation.
- The underlying cause of Jaundicemust be treated first. Medical management is done in most of the cases which involves treating the underlying infections like Hepatitis, leptospirosis and malaria.
- In cases of Hepatitis induced Jaundice, Anti-viral medications are preferred. Malaria can be treated with antibiotics and hydroxychloroquine and quinolones. Newer antivirals are available in treating Hepatitis B & C.
- Bed rest, Nutritious diet, glucose and fruit drinks are recommended. Certain lifestyle changes can be done like regular exercise.
- Special diet avoiding certain foods can be taken in patients with G6PD deficiency.
- Drugs such as Hypnotics, Sedatives and Alcohol must be avoided. Oral Contraceptive Pills used by women must be discontinued till the symptoms are decreased.
- Corticosteroids help to improve the symptoms of autoimmune hemolytic anemia. Hydroxyurea is prescribed for patients with sickle cell anemia.
- Blood transfusions are given to patients suffering from severe hemolytic anemia. If all the other treatments have failed, plasmapheresis is suggested to the patient.
- Iron Supplements and Iron rich foods must be taken in cases of anemia induced Jaundice.
- surgery of the Gall Bladder can reduce the itchiness in the body in severe cases.
- In Newborns, Jaundice can be treated with PHOTOTHERAPY (Light Therapy where the baby is placed under an artificial blue light or the baby can be exposed directly under morning sunlight for a few minutes) and EXCHANGE TRANSFUSION if bilirubin levels are greater than 421mg/dL.
- People with hepatitis A, B, and C infections are advised to have protected sexual intercourse.
- Intravenous immunoglobulin and bone marrow transplantation are done as required in a few genetic disorders causing Jaundice.
- ERCP (Endoscopic retrograde cholangiopancreatography) is the treatment of choice in Extrahepatic Bileduct obstruction (Gallstones; bileduct Malignancy; Pancreatic Malignancy).
- In severe cases, like Bile duct obstruction, surgical management is preferred over medical management. The diseased part of the liver is removed without affecting the function of the liver.
- In severe cases when none of the above treatments have failed, liver transplantation can be done.
Jaundice can be prevented by
- Avoiding alcohol and sedatives drugs like hypnotics, and paracetamol.
- Balanced diet is important to prevent Jaundice (Iron rich foods are to be taken by people with Jaundice induced by anemia).
- Regular Exercise must be done.
- In patients with a family history of Crigler-Najjar syndrome, genetic counselling can be given.
- Patients and the family members must be educated about the possible signs and symptoms seen in the patient and to report any changes immediately.
- Protected sexual intercourse is advised in people with hepatitis A,B,C infections.
- Travelling to any country or region where Hepatitis or malaria is prevalent must be avoided.
- Exposure to any harmful chemicals that can affect the liver must be avoided.
1) Can jaundice be cured?
Yes, Jaundice can be cured. If it is caused due to underlying infection, your doctor may suggest medical management. But in severe cases and if it occurs due to obstruction, then surgery is suggested.
2) Is jaundice serious?
Jaundice is serious only when bilirubin levels are very high in the body and it may cause complications like liver failure, sepsis and death.
3) How long will it take to get jaundice cured?
The treatment of jaundice depends on the underlying conditions. In newborns, it disappears after 2 weeks of life.
Apollo Hospitals has the Best Gastroenterologist in India. To find the best gastroenterologist doctors in your nearby city, visit the links below:
- Gastroenterologist in Bangalore
- Gastroenterologist in Chennai
- Gastroenterologist in Hyderabad
- Gastroenterologist in Delhi
- Gastroenterologist in Mumbai
- Gastroenterologist in Kolkata
© Copyright 2024. Apollo Hospitals Group. All Rights Reserved.
Hello, Guest!
Quick login using Mobile Number.
 +91 8069991061
Book Health Check-up
+91 8069991061
Book Health Check-up