






.png)


What are salivary glands?
The salivary glands are located around the mouth. The saliva they produce moistens food to help with chewing and swallowing. It contains enzymes that begin the digestion process, and help cleanse the mouth by washing away bacteria and food particles.
Where are they located?
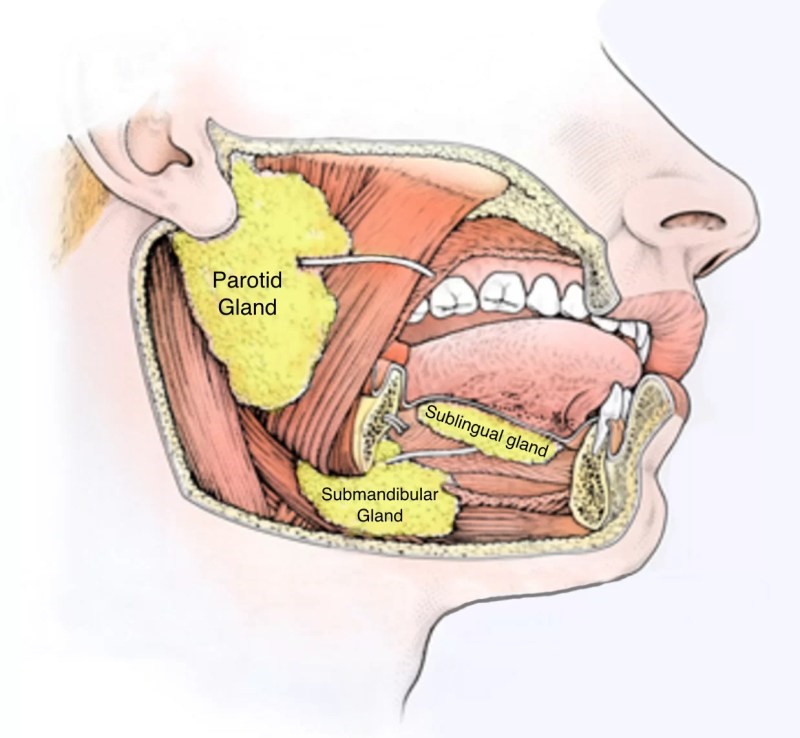
Fig.1. Major salivary glands
There are three pairs of major salivary glands(Fig.1). The largest are the parotid glands, located in each cheek over the jaw in front of the ears. Two submandibular glands are at the back of the mouth on both sides of the jaw. Two sublingual glands are under the floor of the mouth. There are also thousands of minor salivary glands and are widely distributed in the mucosa of the lips, cheeks, hard and soft palate, uvula, floor of mouth, tongue, and peritonsillar region.
What type of tumours occur in salivary glands?
About 85% of salivary gland tumours occur in the parotid glands, followed by the submandibular and minor salivary glands, and about 1% occur in the sublingual glands. About 75 to 80% are benign, slow-growing, movable, painless, usually solitary nodules beneath normal skin or mucosa. Occasionally, when cystic, they are soft but most often they are firm.
Benign Tumours
The most common type is a pleomorphic adenoma (mixed tumour). They are slow-growing and lobular and may become very large without interfering with facial nerve function. Malignant transformation is possible, resulting in carcinoma ex pleomorphic adenoma, but this usually occurs only after the benign tumour has been present for more than a decade. Other benign tumours include monomorphic adenoma, oncocytoma, and papillary cystadenoma lymphomatosum (warthin’s tumour). These tumours rarely recur and rarely become malignant.
Malignant Salivary Gland Tumours:
Malignant tumours are less common and are characterized by rapid growth or a sudden growth spurt. They are firm, nodular, and can be fixed to adjacent tissue. Pain and neural involvement (facial nerve paralysis) are common. Eventually, the overlying skin or mucosa may become ulcerated or the adjacent tissues may become invaded. Surgery, followed by radiation therapy, is the treatment of choice for resectable disease. Currently, there is no effective chemotherapy for salivary cancer.
Mucoepidermoid carcinoma in their 20s to 50s. It can manifest in any salivary gland, often in a minor salivary gland of the palate. Intermediate and high-grade mucoepidermoid carcinomas may metastasize to the regional lymphatics, which must be addressed with surgical dissection or postoperative radiation therapy.
Adenoid cystic carcinoma
incidence is between ages 40 and 60, and symptoms include severe pain and, often, facial nerve paralysis. It has a propensity for perineural invasion and spread, with disease potentially extending many centimetres from the main tumour mass. Lymphatic spread is not a common feature of this tumour, so elective nodal treatment is less common. Pulmonary metastases are common, although patients can live quite long with them.
Acinic cell carcinoma,
a common parotid tumour, occurs in people in their 40s and 50s. This carcinoma has a more indolent course, as well as an incidence of multifocality.
Carcinoma ex pleomorphic adenoma
is adenocarcinoma arising in a pre-existing benign tumour. Only the carcinomatous element metastasizes.
What symptoms does it cause?
Most benign and malignant tumours manifest as a painless mass in front of the ears, under the chin, or on the floor of the mouth. However, malignant tumours may invade nerves, causing localized or regional pain, numbness, paraesthesia, or a loss of motor function (facial paralysis). Sudden onset of pain, increase in size and facial palsy should raise the suspicion of malignancy.
How is it diagnosed?
- Needle biopsy
- CT and MRI for knowing the extent of disease
- CT and MRI locate the tumour and describe its extent. Biopsy confirms the cell type. A search for spread to regional nodes or distant metastases in the lung, liver, bone, or brain may be indicated before treatment is selected.
How is it treated?
Surgery:
Treatment of benign tumours is surgery. The aim of the operation is to completely excise the tumour with an adequate margin of normal tissue and preserve the facial nerve and its branches. There are lots of variations in the branching of extracranial facial nerve (Fig.2). Magnification with surgical loupe (Fig.3) or microscope helps in identification as well as preservation of facial nerve and its branches. Facial nerve monitoring (Fig.4) is a simple, effective adjunct method that is available to surgeons to assist with the functional preservation of the facial nerve during parotid surgery.
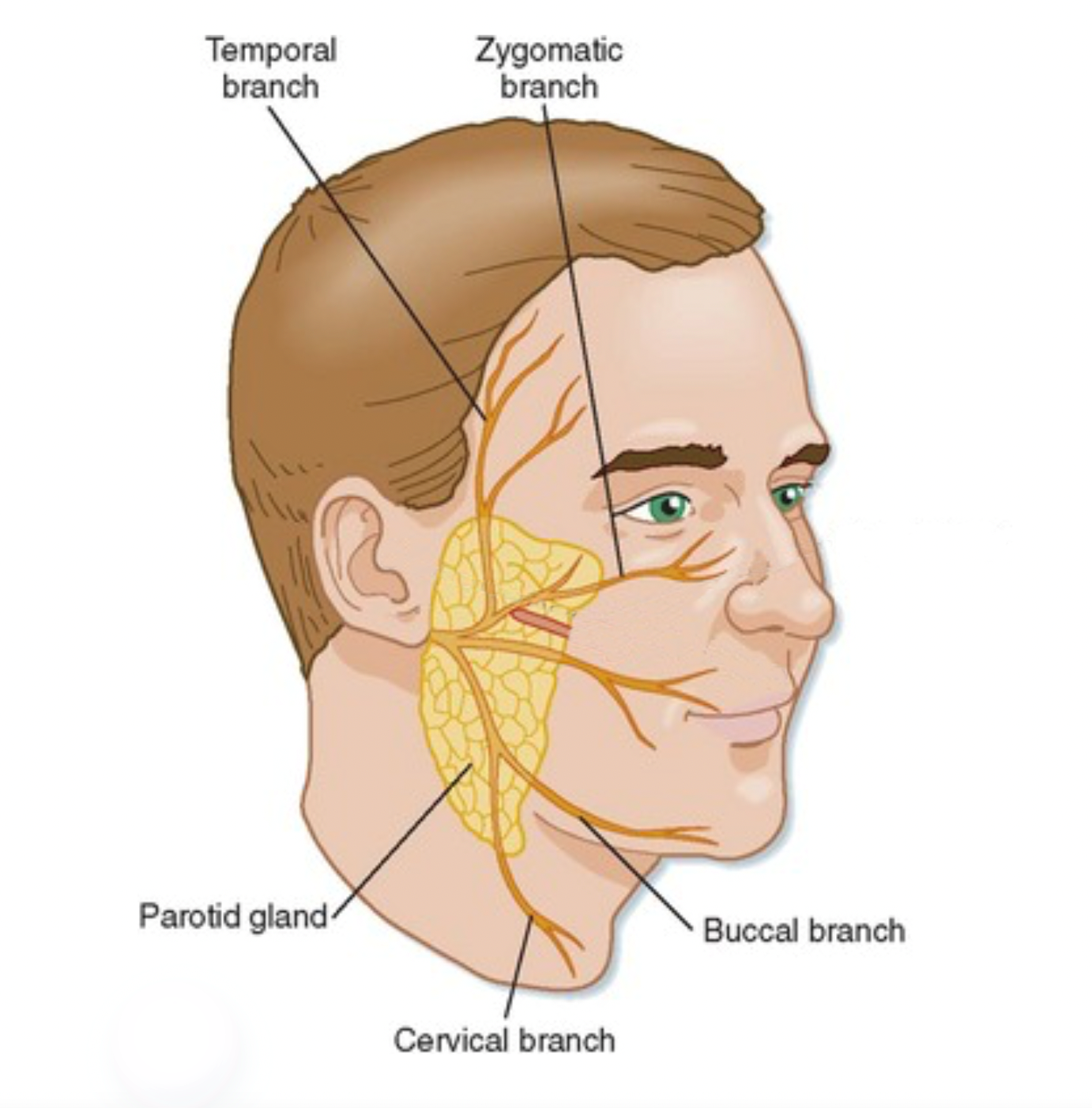
Fig.2. Anatomic variations in the branching of the extracranial facial nerve

Fig.3. Surgical loupe

Fig.4. Electrophysiological monitoring
Although pleomorphic adenomas are benign, they will recur after surgery unless they are completely removed. Enucleation is inadequate and the tumour recurs. When tumour recurs in the parotid region, the facial nerve is at greater risk from damage during re-operation than it was during the initial procedure. Therefore, tumour must be removed with a cuff of normal parotid tissue all around (adequate parotidectomy, superficial parotidectomy and total conservative parotidectomy).
Parotidectomy
When the tumour is in the superficial lobe, the tumour is removed along with the superficial lobe of parotid gland (Superficial Parotidectomy) after identifying and preserving the facial nerve and its branches. When a tumour arises in the parotid gland deep to the facial nerve (deep lobe tumour), the portion of the parotid gland superficial to the facial nerve is elevated or removed, the facial nerve is then dissected off the deep lobe containing the tumour, and finally the tumour deep to the nerve is removed along with the remaining parotid tissue. Benign tumours of the submandibular gland require total removal of the gland for diagnosis and treatment.
Surgical treatment for malignant tumours of the parotid depends on its extent. Unless the patient has facial nerve paralysis before surgery or the nerve is found to be directly invaded or surrounded by malignant tumour at surgery, it is preserved. When the facial nerve must be divided, it is repaired. The facial nerve can be reconstructed using a nerve graft, e.g., the greater auricular or sural nerve. It takes many months for the facial function to recover. If the proximal segment of the facial nerve is not available for grafting, the distal segment or branches of the facial nerve is connected (anastamosis) to the hypoglossal nerve or to the nerve to masseter muscle, either directly or with a nerve graft.
For low-grade salivary gland cancers, complete excision is sufficient treatment. For high-grade cancers, postoperative radiation therapy is indicated for site of the primary cancer and regional lymph nodes. Clinically involved lymph nodes are removed by a radical or modified neck dissection.
Radiation Therapy: In cases where complete surgical removal is challenging or when dealing with malignant tumours, radiation therapy may be employed to target and destroy cancer cells after surgery.
Chemotherapy: Systemic chemotherapy is occasionally used, particularly for aggressive and metastatic salivary gland tumours. However, its efficacy can vary depending on the tumour type.
Post-Treatment Life and Follow-Up Care for Salivary Gland Tumours
After undergoing treatment for salivary gland tumours, a crucial aspect is regular follow-up care to monitor recovery progress and identify potential recurrence. This involves routine check-ups and medical assessments to ensure ongoing well-being, specialized rehabilitation if needed, and the adoption of a healthy lifestyle to promote holistic well-being.
Conclusion
Understanding salivary gland tumours, their prevention, diagnosis, and treatment is crucial for overall health. Early detection significantly improves the chances of successful treatment. Adopting a healthy lifestyle and staying vigilant for symptoms contribute to reducing the risk of these tumours. With advancements in medical technology and comprehensive care, individuals diagnosed with salivary gland tumours can look forward to a positive and healthy life post-treatment.

Dr. C. Rayappa, FRCS
Senior Consultant – Head & Neck Oncology and Skull Base Surgery
Apollo Cancer Centre, Chennai

Dr. C. Rayappa, FRCS Senior Consultant – Head & Neck Oncology and Skull Base Surgery-Apollo Cancer Centre, Chennai



